
What is ADHD?
Attention Deficit Hyperactivity Disorder, better known as ADHD, is one of the most common childhood neurodevelopmental conditions, and it is often at the center of questions from parents trying to understand what is happening in their child’s brain because of their behaviors. Children with ADHD may struggle to sit still, stay focused, follow directions, or think before acting, and those challenges can affect school performance, friendships, and family life. While many children show some of these behaviors occasionally, ADHD is different because the symptoms are persistent, occur across multiple settings, and interfere with daily functioning in a meaningful way. For many families, stimulant medication becomes part of the conversation because it is one of the most effective ways to reduce these symptoms [4, 14]. To understand why these medications might be helpful, we need to explore the brain regions associated with ADHD.
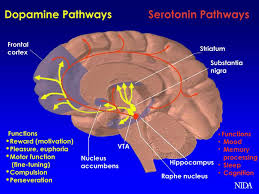
In children with ADHD, the messaging systems involved in attention, planning, and impulse control may not be working as efficiently as they should, especially in a part of the brain called the prefrontal cortex. This region is responsible for executive functions such as organization, working memory, emotional regulation, and the ability to delay gratification. It acts almost like a control center, helping individuals prioritize tasks, ignore distractions, and make thoughtful decisions rather than impulsive ones. When this region is not functioning optimally, it can become much harder for a child to manage behaviors that others might take for granted. Tasks like sitting through a lesson, completing homework, or waiting their turn in a conversation can require significantly more effort. When these circuits are out of sync, everyday tasks that require waiting, focusing, or shifting attention can feel much harder [2].
The Chemistry of Focus
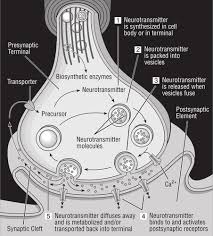
But how do these brain regions talk to one another. Brain cells, or neurons, do not directly touch one another. Instead, they communicate across tiny gaps called synapses. When one neuron activates, it releases chemical messengers, known as neurotransmitters, into the synapse. These chemicals then bind to receptors on the next neuron, sending the signal along the desired path. After the connection is made, the neurotransmitters need to be removed from the space so that signals remain discreet and clear. They are either broken down or recycled into the original neuron through a process called reuptake. This system allows the brain to send precise, controlled signals that regulate everything from movement to decision-making. Individuals diagnosed with ADHD appear to have an imbalance in some of these neurotransmitters in the brain.
Two neurotransmitters are especially important in ADHD: dopamine and norepinephrine. Dopamine helps regulate motivation, attention, and reward, and it plays a key role in reinforcing behaviors by signaling when something is important or worth repeating. Norepinephrine, on the other hand, affects alertness, arousal, and the body’s response to stress. It helps the brain stay focused and ready to respond to incoming information [2, 13]. In many children with ADHD, these chemicals are not available in the right amount or at the right time in key brain regions, particularly in the prefrontal cortex and related networks [2].
This imbalance can make it harder to stay on task, resist impulses, or ignore distractions. For example, if dopamine signaling is too low, tasks that are not immediately rewarding—like homework or chores—may feel almost impossible to engage with. The brain is essentially under-stimulated in areas responsible for attention and motivation, leading the child to seek out more stimulating activities instead. Similarly, disruptions in norepinephrine signaling can make it difficult to maintain consistent attention or regulate emotional responses. As a result, a child may seem “out of control” or “spacey,” when in fact the brain is struggling to communicate effectively. Understanding this helps explain why ADHD is not just about willpower or discipline, but about how the brain is wired and how it uses chemicals to send signals [12].
Brain imaging studies have supported this understanding by showing differences in activity (signals between cells in the brain) and connectivity (patterned connections within the brain used for performing repeated tasks) in individuals with ADHD. Functional imaging techniques, such as fMRI and PET scans, have demonstrated that the prefrontal cortex which is involved in attention and executive function may be less active or less coordinated. These findings do not mean that the brain is damaged, but rather that it is developing and functioning in a different way [8]. This difference in brain activity helps explain why traditional discipline strategies alone are often not enough to address ADHD symptoms. Instead, treatments that target the underlying neurobiology, including medication, can play a critical role.
Medication modification
Stimulant medications such as Adderall, Vyvanse, and Focalin work by increasing the amount of dopamine and norepinephrine available in the brain. They do this mainly by blocking the recycling process that normally removes these chemicals from the synapse. By blocking recycling, the neurotransmitters remain active longer and can keep sending their signal. In some cases, like with amphetamine-based medications, the drugs also encourage the release of dopamine, giving the brain a stronger chemical boost in the areas that need it most [6]. Methylphenidate-based medications (Ritalin) primarily block reuptake, while amphetamine-based medications (Adderall) both block reuptake and increase release, which can lead to slightly different effects between individuals.
The use of medication is not a cure but helps create a more efficient communication system in the brain circuits that help a child pay attention, manage impulses, and stay on task [3,12]. In many cases, that can feel like a major shift in everyday life. Tasks that once felt overwhelming may become more manageable, and the child may be better able to organize their thoughts and actions. It is important to note that these medications do not “add” new abilities but rather help the brain use its existing abilities more effectively [9].
Benefits and Trade-Offs
For parents, the benefits of stimulant medication are often seen in practical, everyday ways. A child may be able to finish homework with less frustration, follow classroom instructions more consistently, or make it through a school day with fewer behavioral struggles. Teachers may report that the child is more engaged during lessons, raises their hand instead of calling out, and is better able to complete assignments on time. At home, routines may become smoother, and daily tasks like getting dressed, cleaning up, or transitioning from one activity to another may feel less overwhelming. Some children also become less impulsive and more able to think before they act, which can improve relationships with siblings, classmates, and adults. These changes can be meaningful not only because symptoms improve, but because life starts to feel a little more manageable for the whole family [4,7].
For many children, the relief that comes with better symptom control is not just clinical; it is emotional. A child who has been constantly corrected for not paying attention, for not finishing work, or for blurting out answers may begin to experience more success. Over time, this can lead to improved self-esteem and a more positive sense of identity. They may feel less ashamed, less frustrated, and more confident about their ability to learn and participate. Teachers often notice that children on effective treatment are easier to teach, more cooperative, and more present in the classroom. In that sense, medication does not erase ADHD, but it can help level the playing field so that the child’s strengths have a better chance to show up [14].
At the same time, stimulant medications are not without drawbacks, and it is important for parents to know what to watch for. Some children experience decreased appetite, trouble sleeping, headaches, stomach upset, or irritability [1,11]. These side effects are often mild and can sometimes be managed by adjusting the dose or timing of the medication, but in other cases they may be more disruptive. Some children may feel less energetic or emotionally “flat,” which can be upsetting if the medication seems to change the child’s personality [10,11]. Parents sometimes describe this as their child seeming “not like themselves,” which can be an important signal that the medication or dose may need to be reconsidered.
In some cases, a child may do well at school but struggle with side effects at home, or the medication may wear off too soon and leave the child feeling more difficult in the afternoon or evening. This “rebound” effect can make evenings particularly challenging, especially when homework and family routines still need to be completed. That is why treatment often involves careful follow-up, dose adjustments, and honest conversations between parents and the clinician about what is and is not working [5,14].
Finding the Right Fit
Finding the right medication and dose can take time, and families should be prepared for some trial and error. One child may respond well to methylphenidate-based medication, while another does better on an amphetamine-based one. There is no rhyme or reason, it just depends on the kids brain. Some children need a short-acting formulation that works quickly, while others benefit from a long-acting version that lasts through the school day. The timing and duration of medication can also affect how well it fits into daily life. For example, a child who needs help with homework and evening routines may need a different schedule than one who mainly struggles during school hours. This process can feel frustrating, especially if parents are hoping for a fast and all-encompassing solution, but medication is often part of getting the safest and most effective treatment [14].
There are also personal issues that can matter just as much as the medical ones. Some children do not like the idea of taking medicine every day, especially if they feel different from their friends. Others may worry about taking medication at school or about what others might think. Parents may have their own concerns, too, including questions about long-term use, stigma, cost, or whether medication means they are not doing enough to help behaviorally. Some families may also have cultural or personal beliefs about medication that influence their decision-making. These feelings are normal. ADHD treatment is not just about managing symptoms on a chart; it is about finding an approach that fits the child’s needs, the family’s values, and the realities of everyday life. For that reason, the best treatment decisions usually come from open discussion, regular follow-up, and a willingness to adjust the plan as needed [14].
Support Beyond Medication
In addition to medication, many families find that behavioral strategies, school accommodations, and healthy routines make a meaningful difference. A child may benefit from structured schedules, clear expectations, visual reminders, and positive reinforcement for effort and progress. These strategies help externalize organization and planning, which can be especially helpful for children whose executive functioning skills are still developing. Teachers can support this by using organizational tools, breaking tasks into smaller steps, and allowing extra time when needed. Preferential seating, movement breaks, and individualized instruction can also help children stay engaged in the classroom.
Parents may also help by creating predictable routines, limiting screen time, and encouraging physical activity, which can naturally support attention and mood. Sleep is another critical factor, as many children with ADHD already struggle with sleep regulation, and poor sleep can worsen symptoms. When medication is combined with these supports, children often do best. The goal is to create a “treatment ecosystem” rather than relying on any one strategy alone [5].
It is also important to recognize that medication decisions are not permanent. Families can choose to try medication and reassess overtime, adjusting or discontinuing it if needed. This flexibility can make the decision feel less overwhelming and allows for a more individualized approach. Regular follow-up appointments help ensure that the treatment continues to meet the child’s needs as they grow and their environment changes.
In the end, stimulant medications can be a powerful tool for children with ADHD, but kids with ADHD work best when they are part of a thoughtful, individualized plan. The goal is not simply to quiet a child down, but to help them think more clearly, focus more easily, and move through the day with less struggle. For many families, that can make a real difference. Still, the decision to use medication should always include a careful look at both the benefits and the possible downsides, along with space for the child’s own experience. When medication is used wisely, in partnership with the family and the child, it can become a positive force in the story of ADHD—not the whole story, but an important chapter that helps a child live more fully and confidently.
Refrences
1. ADHD Medications: How They Work & Side Effects. (n.d.). Cleveland Clinic. Retrieved April 28, 2026, from https://my.clevelandclinic.org/health/treatments/11766-adhd-medication
2. Arnsten, A. F. T. (2006a). Fundamentals of attention-deficit/hyperactivity disorder: Circuits and pathways. The Journal of Clinical Psychiatry, 67 Suppl 8, 7–12.
3. Arnsten, A. F. T. (2006b). Stimulants: Therapeutic Actions in ADHD. Neuropsychopharmacology, 31(11), 2376–2383. https://doi.org/10.1038/sj.npp.1301164
4. Cortese, S., Adamo, N., Del Giovane, C., Mohr-Jensen, C., Hayes, A. J., Carucci, S., Atkinson, L. Z., Tessari, L., Banaschewski, T., Coghill, D., Hollis, C., Simonoff, E., Zuddas, A., Barbui, C., Purgato, M., Steinhausen, H.-C., Shokraneh, F., Xia, J., & Cipriani, A. (2018). Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. The Lancet. Psychiatry, 5(9), 727–738. https://doi.org/10.1016/S2215-0366(18)30269-4
5. Cortese, S., Holtmann, M., Banaschewski, T., Buitelaar, J., Coghill, D., Danckaerts, M., Dittmann, R. W., Graham, J., Taylor, E., Sergeant, J., & Group, on behalf of the E. A. G. (2013). Practitioner Review: Current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents. Journal of Child Psychology and Psychiatry, 54(3), 227–246. https://doi.org/10.1111/jcpp.12036
5. Dopamine: What It Is, Function & Symptoms. (n.d.). Cleveland Clinic. Retrieved October 20, 2025, from https://my.clevelandclinic.org/health/articles/22581-dopamine
6. Faraone, S. V. (2018). The Pharmacology of Amphetamine and Methylphenidate: Relevance to the Neurobiology of Attention-Deficit/Hyperactivity Disorder and Other Psychiatric Comorbidities. Neuroscience and Biobehavioral Reviews, 87, 255–270. https://doi.org/10.1016/j.neubiorev.2018.02.001
7. Heins, M. J., Bruggers, I., van Dijk, L., & Korevaar, J. C. (2016). ADHD medication prescription: Effects of child, sibling, parent and general practice characteristics. Journal of Child Health Care, 20(4), 483–493. https://doi.org/10.1177/1367493515620913
8. Peterson, B. S., Potenza, M. N., Wang, Z., Zhu, H., Martin, A., Marsh, R., Plessen, K. J., & Yu, S. (2009). An fMRI Study of the Effects of Psychostimulants on Default-Mode Processing During Stroop Task Performance in Youths With ADHD. The American Journal of Psychiatry, 166(11), 1286–1294. https://doi.org/10.1176/appi.ajp.2009.08050724
9. Swanson, J., Baler, R. D., & Volkow, N. D. (2011). Understanding the Effects of Stimulant Medications on Cognition in Individuals with Attention-Deficit Hyperactivity Disorder: A Decade of Progress. Neuropsychopharmacology, 36(1), 207–226. https://doi.org/10.1038/npp.2010.160
10. Thorell, L. B., & Dahlstrom, K. (2009). Children’s Self-Reports on Perceived Effects on Taking Stimulant Medication for ADHD. Journal of Attention Disorders, 12(5), 460–468. https://doi.org/10.1177/1087054708320430
11. Toomey, S. L., Sox, C. M., Rusinak, D., & Finkelstein, J. A. (2012). Why Do Children With ADHD Discontinue Their Medication? Clinical Pediatrics, 51(8), 763–769. https://doi.org/10.1177/0009922812446744
12. Volkow, N. D., Wang, G., Fowler, J. S., Logan, J., Gerasimov, M., Maynard, L., Ding, Y., Gatley, S. J., Gifford, A., & Franceschi, D. (2001). Therapeutic doses of oral methylphenidate significantly increase extracellular dopamine in the human brain. The Journal of Neuroscience: The Official Journal of the Society for Neuroscience, 21(2), RC121. https://doi.org/10.1523/JNEUROSCI.21-02-j0001.2001
13. Volkow, N. D., Wang, G.-J., Kollins, S. H., Wigal, T. L., Newcorn, J. H., Telang, F., Fowler, J. S., Zhu, W., Logan, J., Ma, Y., Pradhan, K., Wong, C., & Swanson, J. M. (2009). Evaluating Dopamine Reward Pathway in ADHD. JAMA : The Journal of the American Medical Association, 302(10), 1084–1091. https://doi.org/10.1001/jama.2009.1308
14. Wolraich, M. L., Hagan, J. F., Allan, C., Chan, E., Davison, D., Earls, M., Evans, S. W., Flinn, S. K., Froehlich, T., Frost, J., Holbrook, J. R., Lehmann, C. U., Lessin, H. R., Okechukwu, K., Pierce, K. L., Winner, J. D., Zurhellen, W., & SUBCOMMITTEE ON CHILDREN AND ADOLESCENTS WITH ATTENTION-DEFICIT/HYPERACTIVE DISORDER. (2019). Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics, 144(4), e20192528. https://doi.org/10.1542/peds.2019-2528